For decades, the U.S. has spent far more on healthcare than peer countries while delivering similar or worse outcomes.[1] Value-based care (VBC) aims to address cost and quality concerns through moving away from the underlying fee-for-service (FFS) infrastructure, which rewards volume over value. Unlike FFS, VBC assigns risk to hospitals, providers, and/or payers, who are generally rewarded or penalized based on their performance on quality and cost metrics.[2]
Under the Affordable Care Act (ACA), the Center for Medicare and Medicaid Innovation (CMMI) was authorized to test payment models intended to facilitate the transition to VBC.[3] Although these models vary widely in design and implementation, VBC accounted for 44.9% of all healthcare payments in 2025, up from 40% in 2021.[4] Despite its widespread adoption, evidence on VBC’s ability to improve quality while lowering costs remain mixed.[5]
On April 23, 2026, the Center for the Business of Health hosted its annual research symposium, bringing together leaders across policy, practice, industry, and academia to examine whether VBC has delivered on its promises. Through a series of panel discussions, speakers reflected on where VBC has succeeded, where it has fallen short of its aims, and what steps may be necessary to improve cost and quality outcomes. This article summarizes the event’s key takeaways.*
Panelists expressed no clear consensus on how VBC should be defined. While one panelist argued that value-based payments are distinguished by the displacement of risk from the payer to a third party, another contended that VBC describes the goal of delivering value, not the framework required to achieve it. Ultimately, the absence of a shared definition reflects the complexity and misaligned expectations that often sit at the heart of critiques of VBC.
Despite competing definitions of what VBC is today, three key themes emerged for what it should be. First, VBC should impose financial accountability at a scale large enough to change behavior. Second, VBC models should incorporate gaming-proof design to mitigate exploitation. Finally, VBC models should be simple, allowing for easy adoption, implementation, and maintenance.
Panelists generally agreed that VBC has produced limited, if any, gains in quality and cost. Even for the small number of models that have generated savings, panelists questioned their scalability, noting that CMMI pilot results are often not generalizable or scalable. Panelists also noted that reported savings from CMMI models often exclude the costs of implementation and administration, making net savings negligible in many cases.
“If you squinted you might see value, but it’s hardly there.”
Conference participant
VBC commonly identifies utilization, as opposed to price, as the primary driver of U.S. healthcare spending. On average, the U.S. uses less healthcare than peer countries[6] but pays substantially more for individual services.[7],[8] This means that price, not utilization, is at the root of the U.S.’s high health expenditures. Panelists argued that until the U.S. makes price regulation a policy priority, VBC will have limited potential to reduce healthcare spending.
VBC has accelerated horizontal integration across health systems. Implementation of VBC models often requires substantial investment in health information technology (HIT), quality reporting infrastructure, and administrative capabilities. To mitigate this administrative burden, provider organizations have increasingly merged with larger health systems. Despite potential economies of scale, consolidation is commonly associated with higher prices and mixed quality outcomes.[9] As VBC adoption continues to grow, consolidation may undermine the cost and quality improvements at its core.
VBC fails to address the misalignment between price and value. Although healthcare prices are significantly shaped by market forces, reimbursement rates for individual services often do not reflect the value delivered to patients. Primary care is one example of this disconnect: it accounts for 35% of all health visits but only 5% of total spending.[10] Through providing continuous and preventive care, primary care can reduce downstream costs and generate considerable value.[11],[12] Despite these benefits, the Medicare fee schedule** continues to reimburse specialists at substantially higher rates than primary care providers. Additionally, payers often provide limited or no reimbursement for behavioral health practitioners, who are increasingly important in integrated care settings. Without directing payment toward the providers with the greatest potential to create value and reduce downstream costs, VBC may fall short of its aims.
Mandatory CMMI models consistently outperform voluntary ones. Nevertheless, the majority of VBC models currently implemented by CMMI are voluntary. Voluntary models raise concerns about adverse selection, given that organizations that expect to lose money may opt out. These organizations tend to be smaller, rural, and have higher risk patient populations, raising health equity concerns. Together, these limitations reduce the generalizability of CMMI models, as participating organizations are skewed toward particular provider and patient populations.
VBC models can difficult and complex to implement. Administrative fragmentation and complexity are major drivers of U.S. health spending, accounting for 15% to 20% of total expenditures.[13] VBC models add complexity by requiring provider organizations to build data infrastructure and report quality metrics that often vary across payers. Reimbursement frameworks also vary widely across models, contributing to added complexity for organizations implementing multiple models at once. This complexity creates implementation barriers that ultimately reduce participation in VBC.
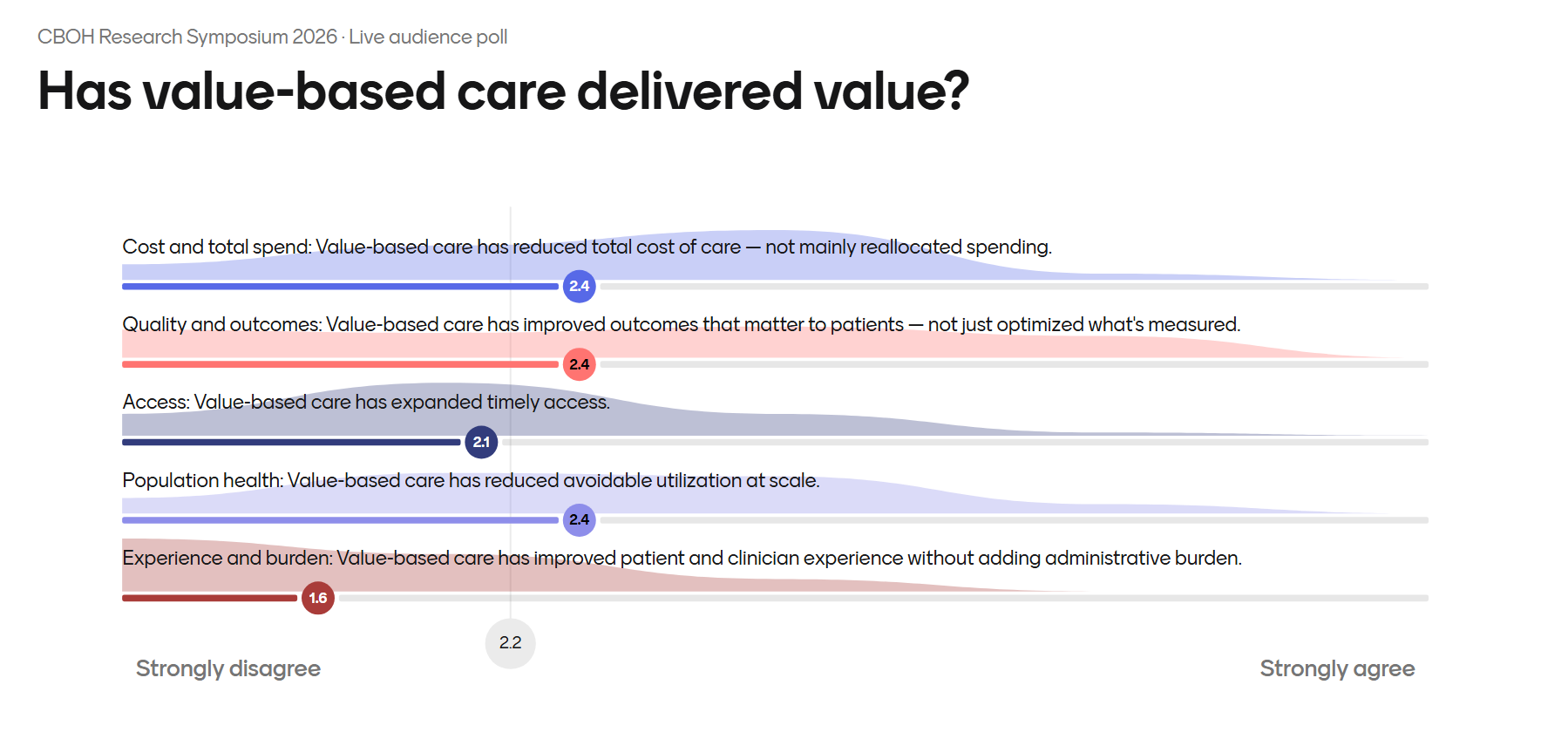
The symposium’s live audience poll (Figure 1) captured this tension. Asked to rate VBC across five dimensions, and invited to revise their answers as the discussion progressed, attendees landed below the neutral midpoint on every measure, averaging 2.2 overall. The lowest score, 1.6 for “experience and burden,” signals where the work remains. Yet the exercise itself reflects the symposium’s central message: honestly assessing where VBC stands is the first step toward making it work.
While panelists debated many aspects of VBC, several recurring themes emerged on how to build on early successes and create the conditions for more of them.
Implementing mandatory participation. Through mandating participation, CMMI can mitigate adverse selection and generate findings that are more generalizable to broader VBC implementation.
Extending the lifetime of VBC models. VBC models implemented over longer periods have been shown to produce stronger results on quality and savings. By contrast, short evaluation horizons create misleading “failure” signals that may undermine opportunities for improvement. Too often, just as an organization has fine-tuned a model and begun to make progress, the model ends, forcing a return to square one. This start-from-scratch loop is a process many provider organizations find daunting.
Eliminating administrative complexity. Seamless implementation of VBC requires alignment of data infrastructure, quality reporting, and reimbursement across payers and providers.
Imposing two-sided risk between payers and providers. To create real financial accountability for patient care, both payers and providers should assume risk. Two-sided risk can drive behavior change and reduce waste.
[1]https://repository.gheli.harvard.edu/repository/14437/
[2]https://www.commonwealthfund.org/publications/explainer/2023/feb/value-based-care-what-it-is-why-its-needed
[3]https://www.kff.org/affordable-care-act/what-is-cmmi-and-11-other-faqs-about-the-cms-innovation-center/
[4]https://hcp-lan.org/apm-measurement-effort-2/
[5]https://www.commonwealthfund.org/publications/explainer/2023/feb/value-based-care-what-it-is-why-its-needed
[6]https://www.commonwealthfund.org/publications/issue-briefs/2023/jan/us-health-care-global-perspective-2022
[7]https://healthcostinstitute.org/all-hcci-reports/international-comparisons-of-health-care-prices-2019/
[8]https://www.healthsystemtracker.org/chart-collection/how-do-healthcare-prices-and-use-in-the-u-s-compare-to-other-countries/
[9]https://www.kff.org/health-costs/what-we-know-about-provider-consolidation/
[10]https://www.nationalacademies.org/read/25983/chapter/1#xvi
[11]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2690145/
[12]https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2724393
[13]https://jamanetwork.com/journals/jama/fullarticle/2785479
*Because all panels operated under the Chatham House Rule, comments in this article are not directly attributed to individual panelists.
**The Medicare fee schedule is often used as a starting point for reimbursement negotiations for non-Medicare beneficiaries. Therefore, even when payers negotiate non-Medicare contracts, the Medicare fee schedule remains highly influential in determining reimbursement rates.
Associate Director, Research, Center for the Business of Health; UNC Kenan-Flagler Business School
Profile Research